Strategies for Success
The Quarterback Model
You are not just a parent. You are the CEO of a small, chaotic non-profit organization called “Your Child’s Health.”
Your job is to:
- Coordinate the care team (psychiatrist, therapist, school, pediatrician)
- Track medications and side effects
- Translate medical jargon for teachers and family
- Advocate when systems fail
This is case management. And you are now a professional.
Building the Care Team
Your teen needs a team, not a single provider. Here’s who should be on it:
The Core Team
- Psychiatrist (Medication management)
- Therapist (Weekly DBT/CBT for mood regulation, coping skills)
- School Counselor or IEP Coordinator (Academic accommodations)
- Pediatrician (Physical health, blood work, growth monitoring)
The Extended Team (If Needed)
- Neuropsychologist (Testing for ADHD/Autism if not yet diagnosed)
- Occupational Therapist (Sensory integration for autistic teens)
- Social Worker (Connecting to community resources, insurance navigation)
- Crisis Team Contact (Mobile crisis unit, hospital liaison)
The Coordinator: YOU
The Problem: These providers don’t talk to each other. The psychiatrist doesn’t know what the therapist is seeing. The school doesn’t know about the new medication.
The Solution: You become the information hub.
Protocol: The Care Team Meeting Agenda
Frequency: Quarterly (every 3 months), or after major changes (new med, hospitalization, IEP update)
Attendees: Psychiatrist, therapist, school counselor, you, your teen (if appropriate)
Format: 30-minute meeting (can be virtual)
Pre-Meeting Prep (What to Bring)
Meeting Agenda Template
1. Check-In (5 min) - “How is [Teen] doing overall?” - Each provider gives 1-minute summary
2. Data Review (10 min) - Share mood chart - Discuss patterns (e.g., “Mood dips every Monday morning—school-related?”) - Review medication compliance and side effects
3. Problem-Solving (10 min) - Identify biggest current challenge (sleep? school? rage episodes?) - Brainstorm adjustments (med change? therapy focus shift? school accommodation?)
4. Action Items (5 min) - WHO will do WHAT by WHEN? - Example: “Dr. Smith will increase Lamictal to 100mg by next week” - Example: “School will implement ‘break card’ by Monday” - Example: “Therapist will work on sleep hygiene for next 4 sessions”
Sample Questions to Ask
- To Psychiatrist: “Should we add/adjust meds based on recent mood data?”
- To Therapist: “What coping skills is [Teen] actually using at home?”
- To School: “Can we add [specific accommodation] to the IEP?”
- To Everyone: “Are we all on the same page about the crisis plan?”
Technology Tools: Outsourcing Your Brain
You cannot remember everything. Use apps and systems.
Mood Tracking
- App: Daylio, eMoods, or simple Google Sheet
- What to Track: Sleep hours, mood (1-10 scale), incidents (rage, crying, self-harm)
- Frequency: Daily (set phone reminder for 8 PM)
- Why: Patterns emerge over weeks. You’ll spot triggers psychiatrist would miss.
Medication Management
- App: Medisafe, Round Health
- Features: Reminders, refill alerts, side effect logs
- Why: Teens forget. Parents forget. Apps don’t.
School Communication
- System: Shared Google Doc with school counselor
- Update: Weekly (Fridays) - Brief summary of teen’s week at home
- Why: School sees half the picture. You see the other half. Share it.
Crisis Contacts (Phone + Paper)
Create a Crisis Card (size of credit card, laminated, in wallet):
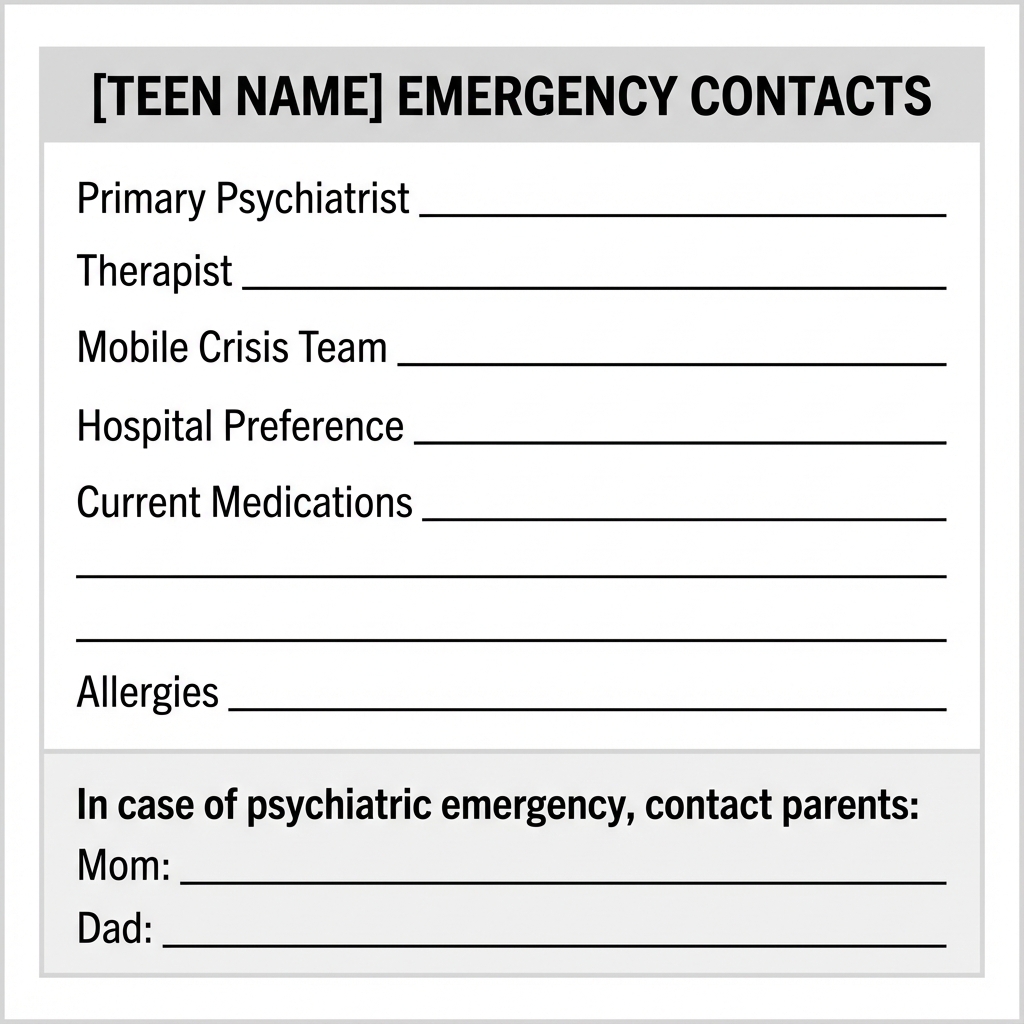
Give copies to: School nurse, grandparents, babysitters, teen (to carry)
School Accommodations: The IEP Cheat Sheet
Your teen’s IEP should address all three conditions (Bipolar, ADHD, Autism). Most schools only address one. Push back.
Executive Function Support (ADHD)
Communication Protocols
Parent → Psychiatrist
When to Contact: - Urgent (call/page): Suicidal ideation, violence, psychosis - Soon (call within 24h): New side effect, 3+ days no sleep - Routine (email/portal): Questions about dosing, refills
What to Include: - Brief summary: “Leo hasn’t slept in 3 days, very irritable, talking fast” - Current dose: “On 900mg Lithium, 100mg Lamictal” - Request: “Should we increase mood stabilizer or bring him in?”
Parent → School
Weekly Update Template (Email):
Subject: [Teen Name] Weekly Update - [Date]
Hi [Counselor Name],
Quick update on [Teen]:
- Mood: Stable this week / Had depressive dip Tue-Thu / Hypomanic energy Mon-Wed
- Sleep: Getting 7hrs average / Only 4hrs last 3 nights
- Medications: No changes / Started new dose [X] on [date]
- Concerns: None / Watch for [specific behavior]
Let me know if you see anything concerning on your end. Thanks!
Parent → Extended Family (Boundaries)
Script:
“We appreciate your concern about [Teen]. We’re working with a team of doctors and following their treatment plan. If you’d like to help, here’s what would be most useful: [specific ask, e.g., ‘Take sibling for afternoon once a week,’ ‘Don’t comment on Teen’s appearance/behavior’]. If that doesn’t work for you, we understand, but we won’t be discussing the treatment plan further.”
Self-Advocacy: Teaching Your Teen
Eventually, your teen needs to manage their own care. Start now (age-appropriately).
Ages 13-14: Awareness
- Teach: Names of medications, why they take them
- Practice: “Can you tell Dr. Smith how you’ve been sleeping?”
- Goal: Teen can describe symptoms to doctor (with you there)
Ages 15-16: Participation
- Teach: Side effects to watch for, when to ask for help
- Practice: Teen calls/texts you when feeling “off”
- Goal: Teen actively participates in doctor visits (not just you talking)
Ages 17-18: Transition Prep
- Teach: How to refill prescriptions, schedule appointments, use insurance
- Practice: Teen makes one appointment on their own (you supervise)
- Goal: Teen can manage care with minimal parent involvement (ready for college/adulthood)
The Takeaway
Success in managing the “Double Diagnosis” requires: 1. A coordinated care team (quarterly meetings, shared information) 2. Technology tools (mood tracking, med reminders, crisis cards) 3. School advocacy (IEPs that address ALL conditions) 4. Clear communication (protocols for when/how to contact providers) 5. Self-advocacy training (age-appropriate independence building)
You are the Quarterback. The plays are complex. The team doesn’t always coordinate. But YOU keep the game moving forward.
And that makes all the difference.