Medical Traffic Jams
The Chemistry Set
Treating the “Double Diagnosis” is like trying to drive a car with one foot on the gas and one foot on the brake.
- The Gas: Stimulants (Ritalin, Adderall, Vyvanse) for ADHD.
- The Brake: Mood Stabilizers (Lithium, Lamictal, Depakote) and Antipsychotics (Seroquel, Risperdal) for Bipolar.
- The Crash: If you hit the gas before the brakes are working, you crash.
Case Study: Leo’s “Stimulant Trap”
Leo Rivera (16) was struggling in school. He couldn’t focus. He was impulsive. The doctor prescribed Vyvanse. “It’s the gold standard for ADHD,” she said. And it worked. Leo’s grades went up. He was cleaning his room. His parents were thrilled. But three months later, the “crash” came. Leo started staying up until 3 AM “organizing” his closet. He became irritable, snapping at his little sister. Then came the rage. He punched a hole in the wall because he couldn’t find his charger. He screamed that his parents were “ruining his life.” The doctor increased the Vyvanse, thinking the ADHD was “worsening.” The Reality: The stimulant was fueling a manic episode. Leo had underlying Bipolar Disorder, and the Vyvanse was acting like rocket fuel. - The Stat: Treating ADHD with stimulants alone in a Bipolar teen increases the risk of manic induction by 6-7 times.
The Medication Breakdown: What You Need to Know
Mood Stabilizers
Lithium (The Gold Standard)
- How It Works: Lithium regulates neurotransmitter release and protects neurons. It’s the only med proven to reduce suicide risk in Bipolar. Pediatric studies confirm its efficacy in stabilizing acute mania in adolescents (Geller et al. 2012).
- The Catch: Narrow therapeutic window. Too little = doesn’t work. Too much = toxic.
- Blood Tests: Required every 3-6 months to monitor levels (0.6-1.2 mEq/L is the target).
- Side Effects: Thirst, frequent urination, tremor, weight gain, acne.
- The Autistic Factor: Many autistic teens hate the “brain fog” feeling. They describe it as “dulling my spark.”
- What to Do: Start at a LOW dose (300mg). Titrate slowly. Negotiate with the teen: “If this makes you feel like a zombie, we’ll try something else.”
Lamictal (Lamotrigine)
- How It Works: Stabilizes glutamate (the “gas pedal” neurotransmitter).
- The Upside: Minimal weight gain, no “dulling” effect. Teens tolerate it better.
- The Danger: The “Rash.” In rare cases (0.1%), Lamictal causes Stevens-Johnson Syndrome, a life-threatening rash.
- The Rule: Titrate SLOW. Start at 25mg and increase every 2 weeks.
- What to Watch: Any rash = STOP immediately and call the doctor.
Lamictal Titration Schedule (8-Week Ramp):
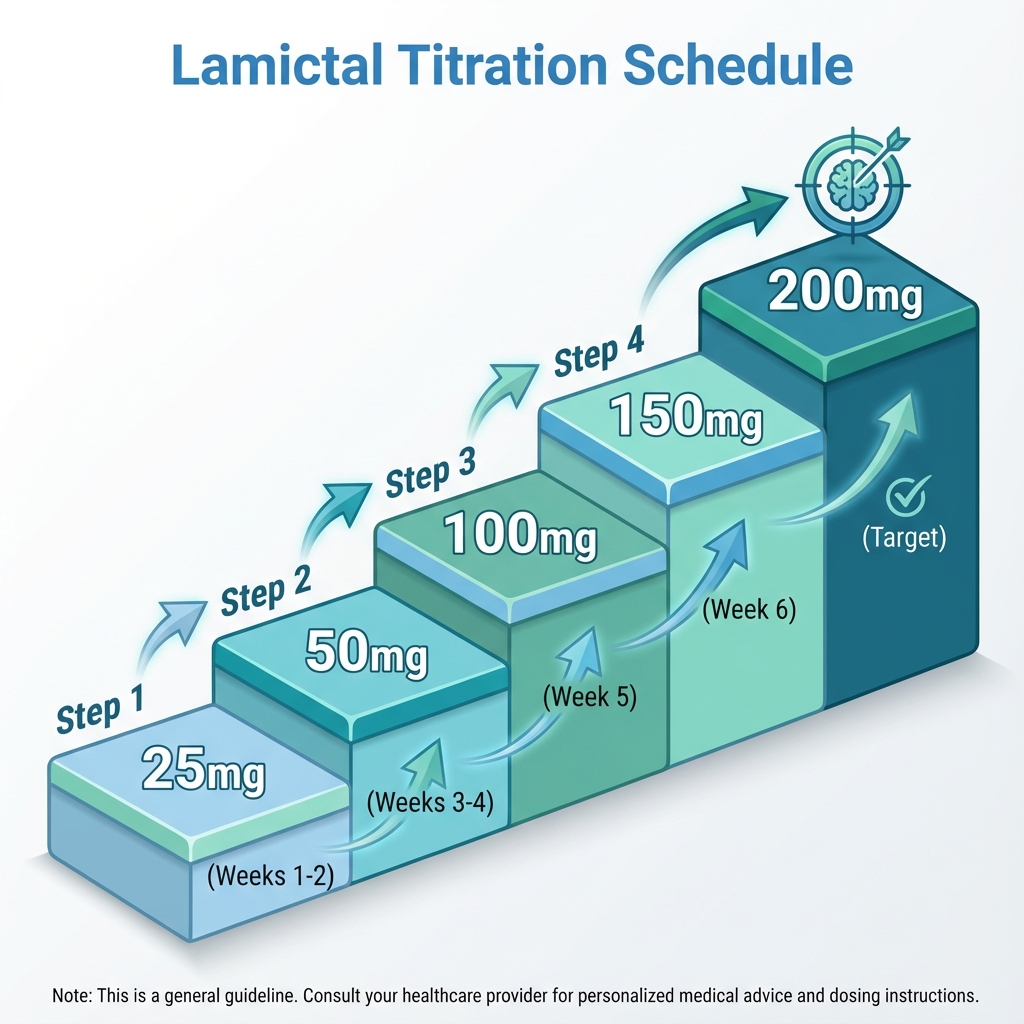
Critical: If a rash appears at ANY point, stop immediately. The slower you titrate, the lower the rash risk.
Depakote (Valproic Acid)
- How It Works: Regulates GABA (the “brake” neurotransmitter).
- The Upside: Fast-acting. Works well for rage.
- The Downside: Weight gain (10-20 lbs common), hair loss, liver toxicity.
- The Autistic Factor: Weight gain can trigger body image issues, especially in teen girls.
Antipsychotics (Atypical)
Seroquel (Quetiapine)
- How It Works: Blocks dopamine receptors. Stops the “power surge” of mania.
- The Upside: Sedating. Great for sleep and acute mania.
- The Downside: Weight gain, metabolic syndrome (diabetes risk).
- The Dose: Low dose (25-100mg) for sleep. High dose (300-800mg) for psychosis.
Risperdal (Risperidone)
- The Danger: Can cause permanent movement disorders (Tardive Dyskinesia) and breast development in boys (gynecomastia).
- When to Use: Only for acute psychosis. Get off ASAP.
Stimulants (The Double-Edged Sword)
The Sequencing Rule
- Stabilize Mood First: 3-6 months on a mood stabilizer with NO cycling.
- Add Stimulant Cautiously: Start with a non-stimulant (Guanfacine, Strattera) first. If that fails, try a LOW-dose stimulant (5mg Adderall).
- Watch Like a Hawk: Any sign of mania (insomnia, rage, grandiosity) = STOP immediately.
Sensory Side Effects: The Autistic Factor
Autistic teens are often “metabolically sensitive.” A dose that is standard for a neurotypical kid might floor an autistic kid. - Texture/Taste: Many autistic teens cannot swallow pills. Liquid formulations or sprinkles are essential. - Interoception: They may feel “weird” or “buzzy” on meds but lack the words to describe it. - The Refusal: When Alex refuses his meds, it’s not “defiance.” It’s because the texture makes him gag, or the “buzzy” feeling triggers his sensory overload.
When Medications Fail
This is the hardest truth: Sometimes, meds don’t work. - Treatment-Resistant Bipolar: 20-30% of people with Bipolar don’t respond to standard meds. - The Options: * Ketamine/Esketamine (Spravato): FDA-approved for treatment-resistant depression. Works in 70% of cases where nothing else did. * ECT (Electroconvulsive Therapy): The most effective treatment for severe, treatment-resistant Bipolar. Modern ECT is safe and painless. It is NOT “One Flew Over the Cuckoo’s Nest.” - The Conversation: “We’ve tried 4 meds and you’re still suffering. I know ECT sounds scary, but it has an 80% success rate. Can we research it together?”
Protocol: The “Start Low, Go Slow” Medication Log
When starting a new med, track these 3 things daily:
- Target Symptom: (e.g., “Focus,” “Rage”) - Rate 1-10.
- Side Effect: (e.g., “Stomach ache,” “Jittery”) - Rate 1-10.
- The “Vibe”: Does the child seem “dull,” “sparky,” or “just right”?
Golden Rule: Change only one variable at a time. Never start two meds in the same week. The Sequencing Rule: 1. Stabilize Mood First: Use Lithium, Lamictal, or an Atypical Antipsychotic to stop the cycling. 2. Treat Focus Second: Only after the mood is stable for 3 months, introduce a low-dose stimulant (or non-stimulant like Guanfacine) and watch like a hawk for mania.